Loculated Pleural Effusion Treatment Guidelines / Pdf Surgical Treatment Of Parapneumonic Pleural Effusion And Its Complications Semantic Scholar - This calls for employment of advanced treatment modalities and development of a standardized.
Loculated Pleural Effusion Treatment Guidelines / Pdf Surgical Treatment Of Parapneumonic Pleural Effusion And Its Complications Semantic Scholar - This calls for employment of advanced treatment modalities and development of a standardized.. Pleural intervention for management of dyspnea. Pleural effusion due cardiovascular disease pleural effusion due to heart failure it is probably the most common cause of pe. A low pleural fluid glucose level (<60mg/dl) is consistent with a complicated parapenumonic effusion or malignancy. The evidence base concerning the management of benign pleural effusions has lagged behind that of malignant pleural effusions in which recent randomised trials are now informing current clinical practice and international guidelines. Parapneumonic effusions should be sampled by thoracentesis.
This calls for employment of advanced treatment modalities and development of a standardized. In patients with chronic, organizing parapneumonic pleural effusions, technically demanding operations may be required to drain loculated pleural fluid and to obliterate the pleural space. Treatment may fail if the catheter is not placed optimally within the loculation or if the fluid is hemorrhagic or fibrinous. In patients with symptomatic mpe and expandable lung undergoing talc pleurodesis, we suggest the use of either talc poudrage or talc slurry. Pleural effusion due cardiovascular disease pleural effusion due to heart failure it is probably the most common cause of pe.
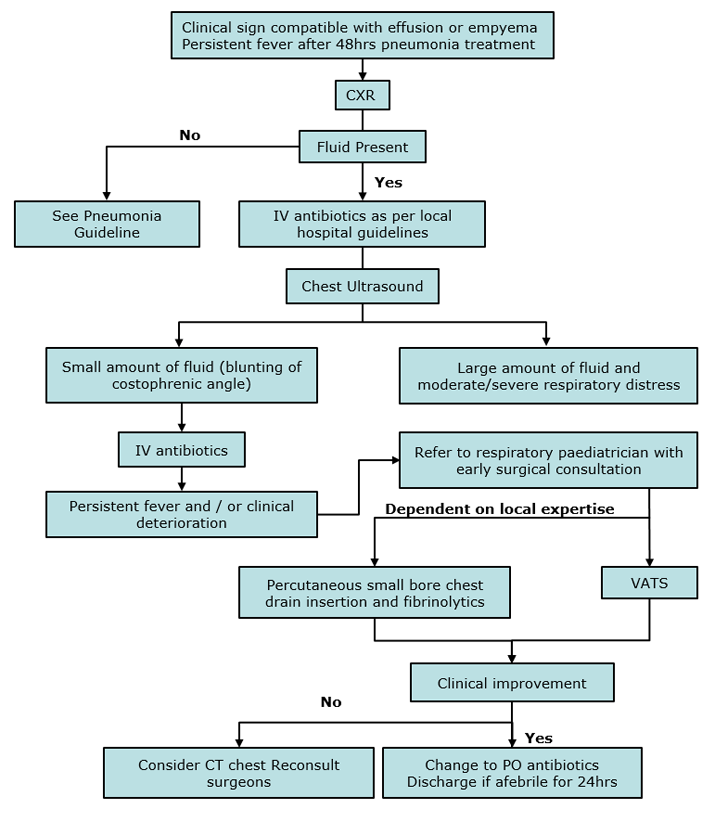
Clinical Practice Guidelines Pleural Effusion And Empyema from www.rch.org.au 10, 23 emergent thoracentesis and/or chest tube placement is necessary in patients with pleural. Change antibiotic only if resistant organism or after discussion with microbiology. Parapneumonic effusion is defined as pleural effusion associated with lung infection (ie, pneumonia). The management of pleural effusion depends on type, stage, and underlying diseases. Pleural effusion predominantly presents with breathlessness, but cough and pleuritic chest pain can be a feature. In patients with symptomatic mpe and expandable lung undergoing talc pleurodesis, we suggest the use of either talc poudrage or talc slurry. The etiology of the pleural effusion determines other signs and symptoms. A pleural effusion describes an excess of fluid in the pleural cavity, usually resulting from an imbalance in the normal rate of pleural fluid production or absorption, or both.
Diuretics and other heart failure medications are used to treat pleural effusion caused by congestive heart failure or other medical causes.
An ultrasound, chest computed tomograp. Empyema fluid generally has a ph of less than 7.2, a glucose level of less than 40mg/dl, and an ldh activity generally over 1,000iu/l. Pleural effusion due cardiovascular disease pleural effusion due to heart failure it is probably the most common cause of pe. Light and rodriguez have proposed a classification and treatment scheme for pleural effusion based on the amount of fluid, gross and biochemical characteristics of fluid, and whether the fluid is loculated.18according to their classification, a transudate is considered as uncomplicated effusion, which can be managed by conservative treatment or antibiotics alone. In patients with symptomatic malignant pleural effusions with nonexpandable lung, failed pleurodesis, or loculated effusion, we suggest the. Pleural intervention for management of dyspnea. Pleural effusions are a common medical problem with more than 50 recognised causes including disease local to the pleura or underlying lung, systemic conditions, organ dysfunction and drugs.1 pleural effusions occur as a result of increased fluid formation and/or reduced fluid resorption. A selective literature search was carried out in medline. The etiology of the pleural effusion determines other signs and symptoms. Change antibiotic only if resistant organism or after discussion with microbiology. Parapneumonic effusions should be sampled by thoracentesis. A pleural effusion describes an excess of fluid in the pleural cavity, usually resulting from an imbalance in the normal rate of pleural fluid production or absorption, or both. Although there is insufficient evidence to support the routine use of this therapy for all parapneumonic effusions/empyemas, fibrinolytic therapy may be considered in patients with loculated pleural effusions, because it may prevent the need for surgical intervention.
Malignant pleural effusions (mpe) are a common pathology, treated by respiratory physicians and thoracic surgeons alike. Parapneumonic effusion is defined as pleural effusion associated with lung infection (ie, pneumonia). Chest tubesprovide continuous drainage in cases of pneumothorax,hemothorax, penetrating chest trauma, complicatedparapneumonic effusion or empyema, or chylothorax.pleural sclerosis (pleurodesis) is usually indicated forpatients with uncontrolled symptomatic malignanteffusions. There has been an increase in the morbidity and mortality associated with parapneumonic effusions and empyema. In patients with chronic, organizing parapneumonic pleural effusions, technically demanding operations may be required to drain loculated pleural fluid and to obliterate the pleural space.
New Ers Eacts Statement On The Management Of Malignant Pleural Effusions Ers European Respiratory Society from mk0ersnetorgsavg5whs.kinstacdn.com Diuretics and other heart failure medications are used to treat pleural effusion caused by congestive heart failure or other medical causes. Chest tubesprovide continuous drainage in cases of pneumothorax,hemothorax, penetrating chest trauma, complicatedparapneumonic effusion or empyema, or chylothorax.pleural sclerosis (pleurodesis) is usually indicated forpatients with uncontrolled symptomatic malignanteffusions. Surgery may be recommended when patients fail medical therapy and/or in case of organized empyema with extensive pleural fibrosis requiring decortication 4, 6. There has been an increase in the morbidity and mortality associated with parapneumonic effusions and empyema. Pleural effusion predominantly presents with breathlessness, but cough and pleuritic chest pain can be a feature. 10, 23 emergent thoracentesis and/or chest tube placement is necessary in patients with pleural. The management of pleural effusion depends on type, stage, and underlying diseases. Treatment depends on the severity and the cause.thoracentesis is done to relieve symptoms.
47 the pe occupies only a third (sometimes less) of the hemithorax in more than 80%.
10, 23 emergent thoracentesis and/or chest tube placement is necessary in patients with pleural. A pleural effusion describes an excess of fluid in the pleural cavity, usually resulting from an imbalance in the normal rate of pleural fluid production or absorption, or both. In patients with symptomatic mpe and expandable lung undergoing talc pleurodesis, we suggest the use of either talc poudrage or talc slurry. The causes of benign pleural effusions are broad, heterogenous and patients may benefit from individualised management targeted at both treating the underlying. Surgical thoracostomy tube placement and radiologically guided catheter drainage are standard therapy for loculated pleural fluid collections. This calls for employment of advanced treatment modalities and development of a standardized. Malignant pleural effusions (mpe) are a common pathology, treated by respiratory physicians and thoracic surgeons alike. Empyema fluid generally has a ph of less than 7.2, a glucose level of less than 40mg/dl, and an ldh activity generally over 1,000iu/l. An ultrasound, chest computed tomograp. Surgery may be recommended when patients fail medical therapy and/or in case of organized empyema with extensive pleural fibrosis requiring decortication 4, 6. Treatment depends on the severity and the cause.thoracentesis is done to relieve symptoms. There was one small study that randomized 20 patients with either a loculated pleural effusion or a pleural fluid ph of less than 7.20 to receive either chest tube drainage plus streptokinase or thoracoscopy (43). A pleural fluid ph <7.2 is the single most powerful indicator to predict a need for chest.
Presence of an effusion can complicate the diagnosis as well as the management of infection in lungs and pleural space. The management of pleural effusion depends on type, stage, and underlying diseases. Pleural effusion predominantly presents with breathlessness, but cough and pleuritic chest pain can be a feature. The causes of benign pleural effusions are broad, heterogenous and patients may benefit from individualised management targeted at both treating the underlying. The evidence base concerning the management of benign pleural effusions has lagged behind that of malignant pleural effusions in which recent randomised trials are now informing current clinical practice and international guidelines.
Recommendations Of Diagnosis And Treatment Of Pleural Effusion Update Archivos De Bronconeumologia from multimedia.elsevier.es Surgical thoracostomy tube placement and radiologically guided catheter drainage are standard therapy for loculated pleural fluid collections. Pleural effusions are a common medical problem with more than 50 recognised causes including disease local to the pleura or underlying lung, systemic conditions, organ dysfunction and drugs.1 pleural effusions occur as a result of increased fluid formation and/or reduced fluid resorption. These effusions result from the spread of inflammation and infection to the pleura. The etiology of the pleural effusion determines other signs and symptoms. A pleural fluid ph <7.2 is the single most powerful indicator to predict a need for chest. Presence of an effusion can complicate the diagnosis as well as the management of infection in lungs and pleural space. The level of ldh is correlated with the degree of pleural inflammation. An ultrasound, chest computed tomograp.
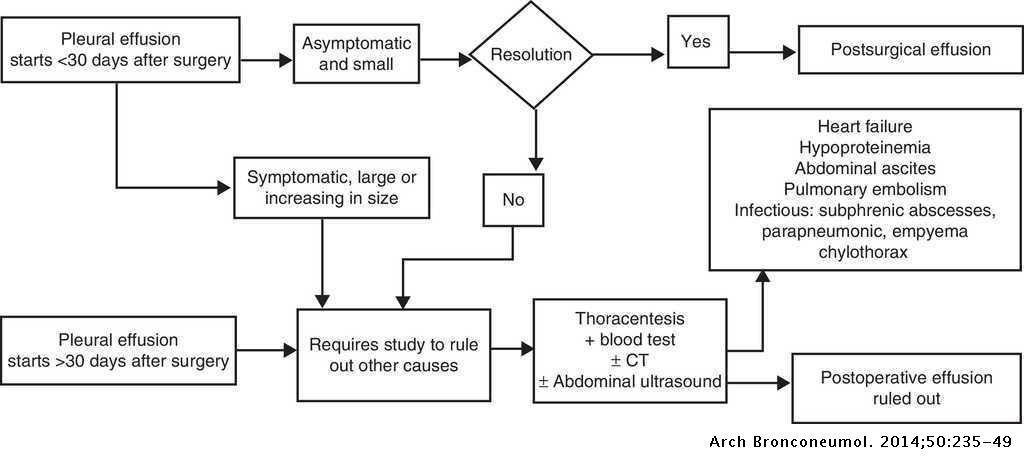
The etiology, prevention and therapy of persistent pleural effusion after thoracic surgical interventions are presented.
International guidelines suggest antibiotic therapy and early drainage of the pleural space by chest tube; A pleural fluid ph <7.2 is the single most powerful indicator to predict a need for chest. Pleural effusions can present in 40% of patients with pneumonia. Pleural effusions are a common medical problem with more than 50 recognised causes including disease local to the pleura or underlying lung, systemic conditions, organ dysfunction and drugs.1 pleural effusions occur as a result of increased fluid formation and/or reduced fluid resorption. Much less commonly, infections in other areas adjacent to the pleura, such as the retropharyngeal, vertebral, abdominal, and retroperitoneal spaces, may spread. A mild idiopathic effusion (<10 mm) is usually. Surgical thoracostomy tube placement and radiologically guided catheter drainage are standard therapy for loculated pleural fluid collections. Persistent postoperative pleural effusion can occur after thoracic surgery and might lead to progressive dyspnea with a subsequent complicated and prolonged hospital stay. Diuretics and other heart failure medications are used to treat pleural effusion caused by congestive heart failure or other medical causes. A selective literature search was carried out in medline. Chest tubesprovide continuous drainage in cases of pneumothorax,hemothorax, penetrating chest trauma, complicatedparapneumonic effusion or empyema, or chylothorax.pleural sclerosis (pleurodesis) is usually indicated forpatients with uncontrolled symptomatic malignanteffusions. A low pleural fluid glucose level (<60mg/dl) is consistent with a complicated parapenumonic effusion or malignancy. The etiology, prevention and therapy of persistent pleural effusion after thoracic surgical interventions are presented.
Much less commonly, infections in other areas adjacent to the pleura, such as the retropharyngeal, vertebral, abdominal, and retroperitoneal spaces, may spread loculated pleural effusion. In patients with chronic, organizing parapneumonic pleural effusions, technically demanding operations may be required to drain loculated pleural fluid and to obliterate the pleural space.


Posting Komentar
0 Komentar